Orthosis for Brachial Plexus Injuries
Creating a prototype to assist with complete brachial plexus injuries
Abstract
What is a Traumatic Brachial Plexus Injury?
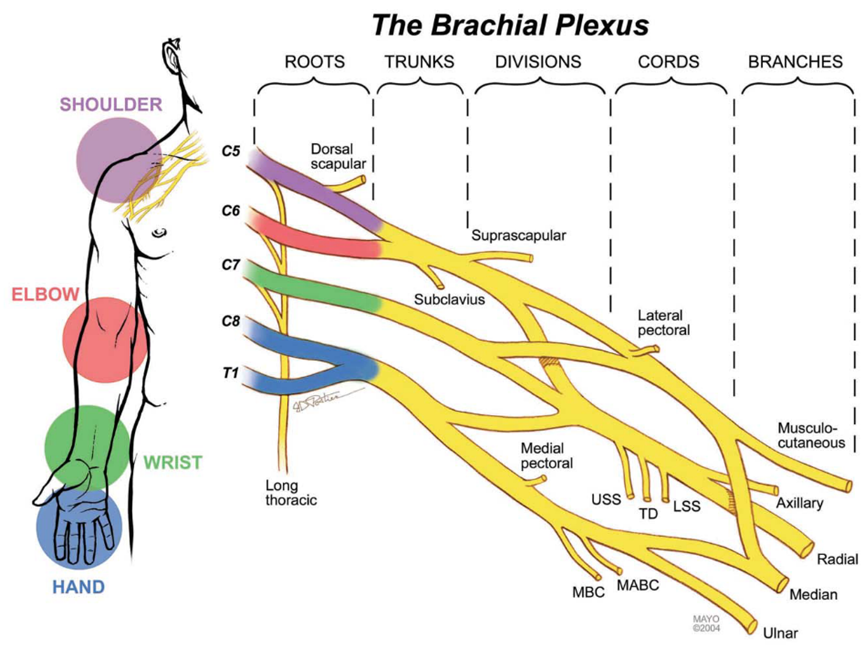
The brachial plexus is the most complex structure in the peripheral nervous system (PNS), and it controls all parts of the upper extremity.1 It is a network of nerves that start in a series of spinal vertebrae. The brachial plexus has roots in the cervical vertebra 5 through the thoracic vertebra 1, denoted as C5, C6, C7, C8, T1.2 A visualization of this anatomy as well as the parts of the upper extremity each nerve root controls can be seen below in Figure 1.
Traumatic brachial plexus injuries (BPIs) occur when some form of stress is applied to the brachial plexus, leading to damage of the structure. The most common cause of traumatic BPIs is high speed motorcycle accidents, during which the arm is pulled harshly away from the body.3 BPIs have severe effects on the function of the upper limb. In complete BPIs, an injury that damages all five roots of the brachial plexus (C5-T1), all parts of the limb can be left completely flail.4
What Issues Arise with Complete BPIs?
Prehension (also termed as grasp) is a key function needed for many activities of daily living (ADLs). Functional prehension is almost always totally lost after a complete BPI. The loss of this function can have severe negative impacts on an individual’s ability to perform key ADLs.5 There is a need to restore prehension after complete BPIs.
What are the Limitations of Current Treatments and Solutions?
Current treatments of complete BPIs result in limited outcomes for critical hand functions such as prehension. The most common treatment method of complete BPIs is surgical reconstruction. A well-established reconstruction method has been published by the Mayo Clinic. This method is outlined below in Figure 2.
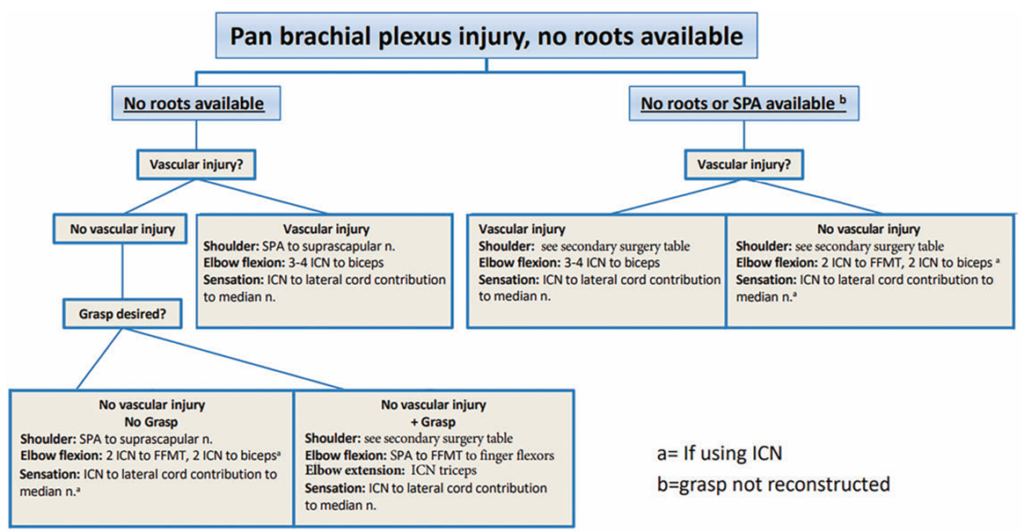
Surgical reconstruction has positive outcomes for elbow function, limited outcomes for shoulder function, and limited to no functional outcomes for hand function and grasping.4 A large factor contributing to these poor outcomes is the distance of the hand from the roots of the brachial plexus. The site of the nerve damage is so far away from the nerves of the hand that nerve regeneration after surgery is too slow to reach the hand before the muscles atrophy.6 Overall, surgery cannot recover functional prehension.
After surgical reconstruction, orthoses are the next treatment for complete BPIs. Existing orthoses have limited functional outcomes for prehension for multiple reasons. Most common orthoses are designed to support the limb without assisting in function.4 Examples of orthoses such as this include the Wilmer Carrying Orthosis and the intrinsic plus resting hand orthosis, which can be seen below in Figures 3 and 4.


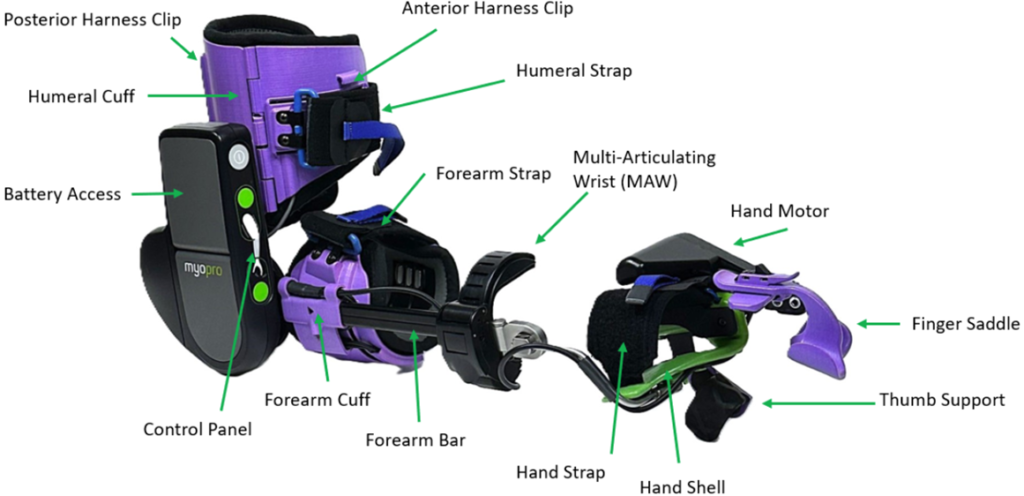
Existing orthoses that do actively assist with function are too bulky for the limb to carry after a compete BPI. The limb is greatly weakened after a BPI; even after surgical reconstruction, the recovered muscle function is still less than that of a healthy arm.7 Therefore, bulky assistive orthoses, such as the MyoPro seen in Figure 5, are not usable by individuals after a complete BPI.
Overall, existing orthoses do not solve the issue of lack of prehension after complete BPIs. In order to recover prehension, an assistive orthosis that meets the unique needs of individuals with complete BPIs is needed. That is the goal of this project.
What is the Solution?
The orthosis will need to consider the unique needs presented by a complete BPI. The musculature of the arm will be weakened, so the design must be lightweight. The arm will lack clear surface electromyography (sEMG) signals, the most common signal used to activate assistive devices. Due to the lack of sEMG signals, activation of the device must use a different method. The wrist will be flail, so it will need to be supported by the device. Skin of the arm and hand after injury will be insensate, so the device must protect the skin from injury. A claw hand deformity is common after BPIs, so the device must correct this deformity. An example of a claw hand can be seen below in Figure 6. An anti-claw design prototype can be seen in Figure 7.

People
Weir Biomechatronics Development Laboratory
Current:
- Project Lead: Wendy Dawson
- Richard F. ff. Weir, PhD
Collaborations
Posters & Conference Presentations
Publications
Funding
Patents
News & Media
References
- M. A. Ferrante, “Brachial plexopathies: classification, causes, and consequences,” Muscle Nerve, vol. 30, no. 5, pp. 547-68, Nov 2004, doi: 10.1002/mus.20131.
- S. L. Orebaugh and B. A. Williams, “Brachial plexus anatomy: normal and variant,” Scientific World Journal, vol. 9, pp. 300-12, Apr 28 2009, doi: 10.1100/tsw.2009.39.
- R. Limthongthang, A. Bachoura, P. Songcharoen, and A. L. Osterman, “Adult brachial plexus injury: evaluation and management,” Orthop Clin North Am, vol. 44, no. 4, pp. 591-603, Oct 2013, doi: 10.1016/j.ocl.2013.06.011.
- A. Y. Shin, A. T. Bishop, M. F. Loosbroch, and R. J. Spinner, “A multidisciplinary approach to the management of brachial plexus injuries: experience from the Mayo Clinic over 100 years,” Journal of Hand Surgery (European Volume), vol. 47, no. 11, pp. 1103-1113, 2022, doi: 10.1177/17531934221110733.
- A. Saudabayev, Z. Rysbek, R. Khassenova, and H. A. Varol, “Human grasping database for activities of daily living with depth, color and kinematic data streams,” Sci Data, vol. 5, p. 180101, May 29 2018, doi: 10.1038/sdata.2018.101.
- S. S. Noland, A. T. Bishop, R. J. Spinner, and A. Y. Shin, “Adult Traumatic Brachial Plexus Injuries,” (in eng), J Am Acad Orthop Surg, vol. 27, no. 19, pp. 705-716, Oct 1 2019, doi: 10.5435/jaaos-d-18-00433.
- J. Kuncoro, F. Deapsari, and H. Suroto, “Clinical and functional outcome after different surgical approaches for brachial plexus injuries: Cohort study,” (in eng), Ann Med Surg (Lond), vol. 78, p. 103714, Jun 2022, doi: 10.1016/j.amsu.2022.103714.
- “What is a MyoPro orthosis?” Myomo Inc. https://myomo.com/what-is-a-myopro-orthosis/ (accessed. Mar 3, 2026).
- Y. Hosokawa and H. Oiwa, “Claw hand deformity in longstanding vasculitic neuropathy,” (in eng), Eur J Rheumatol, vol. 8, no. 3, p. 181, Jul 2021, doi: 10.5152/eurjrheum.2020.20032.